-
He kind of addresses this in his Q&A at the bottom
Q: Different countries are testing at different rates. How can you compare the data?
So long as the fraction of actual cases being detected does not change, this does not affect any inference we can make about the growth rate. 35% growth is still 35% growth, whether we measure 100% of the cases or 50%.
If, for example, Italy is detecting 50% of the cases and the US is detecting 25% of cases, this affects any predictions of how far the US is behind Italy At 35% growth, cases double every 2.5 days, so this undersampling would show the US 2.5 days further behind than it really is.
Likely no-one except Korea and Singapore are getting close to 100% of cases. Probably everyone is detecting at least 20% of cases, because those require medical attention. We don't really know what fraction of cases are missed, but the difference in sampling between countries might skew the delays by a few days in either direction.
-
• #55

Had a quick look but couldn't see whether the Our World in Data stuff has been shared. So here it is.
Overview: https://ourworldindata.org/coronavirus
You can also go to more detailed analyses on their own (such as testing per country: https://ourworldindata.org/covid-testing) and choose the places you're interested in.
But it's important to note that the country-specific data is uneven as some things are reported more frequently than others by different countries.
-
Google have launched their data site https://www.google.com/covid19/
Edit: Hmmm. That Google is a shit site... no real stats at all except search trends, and some scraped wikipedia data. The one posted in the prior comment is what I was expecting.
-
NICE guidance on criteria for admissions to critical care was published yesterday
-
Clinical observations from a US respiratory therapist in an ICU in New Orleans
-
Today's deaths by country chart. Trajectory is not looking good for the UK.
Read the guy's Twitter for more graphs and insights: https://twitter.com/jburnmurdoch
-
Aerosol and Surface Stability of SARS-CoV-2 as Compared with SARS-CoV-1 (NEJM 17 March) https://www.nejm.org/doi/full/10.1056/NEJMc2004973?query=featured_home
-
Got a TL;DR ?
edit
SARS-CoV-2 was more stable on plastic and stainless steel than on copper and cardboard, and viable virus was detected up to 72 hours after application to these surfaces (Figure 1A), although the virus titer was greatly reduced (from 103.7 to 100.6 TCID50 per milliliter of medium after 72 hours on plastic and from 103.7 to 100.6 TCID50 per milliliter after 48 hours on stainless steel).
The stability kinetics of SARS-CoV-1 were similar (from 103.4 to 100.7 TCID50 per milliliter after 72 hours on plastic and from 103.6 to 100.6 TCID50 per milliliter after 48 hours on stainless steel).
On copper, no viable SARS-CoV-2 was measured after 4 hours and no viable SARS-CoV-1 was measured after 8 hours. On cardboard, no viable SARS-CoV-2 was measured after 24 hours and no viable SARS-CoV-1 was measured after 8 hours (Figure 1A).
-
Summarised well here
-
I think we can’t yet expect to know for Belgium. The lockdown was too recent.
... Annals of Internal Medicine that calculates that the median incubation period for COVID-19 is just over five days and that 97.5 percent of people who develop symptoms will do so within 11.5 days of infection.
From here:
https://www.sciencedaily.com/releases/2020/03/200317175438.htm -
• #70
It's also worth keeping in mind population density will almost certainly play a role, and Belgium is densely populated (as is England).
Keeping with the spirit of this thread, here's some data: https://ec.europa.eu/eurostat/web/products-eurostat-news/-/DDN-20170406-1?inheritRedirect=true
-
For clarity, Japan can’t be lumped in with South Korea as regards testing or any kind of effectiveness. Statistics about confirmed cases here are utterly meaningless.
I live in Yokohama and there are extremely low levels of testing. The number of cases are almost definitely exponentially higher than any statistics show.
For an illustration:
- South Korea testing as of 20 March = 316, 664
- Japan testing as of today (23 March) = 20,228
To be honest, the measures have been poor to non-existent and the media is seemingly towing the party line by focusing on how bad it is in other countries. Trains are still packed, work from home is ‘encouraged’ (policy doesn’t get followed by many) and people are very much out and about (50,000 people went to an Olympic torch event last weekend). All of this is basically an attempt by the government to make Abe less unpopular and to try to save the Olympics (in my view, won’t happen).
I don’t know what the future holds for Japan and COVID19, but I’m pretty anxious about it (especially with a two month old and 2 and a half year old).
- South Korea testing as of 20 March = 316, 664
-
Didn't realise there was a data thread - this isn't peer reviewed yet, but it's a stab at estimating the actual rate of infection taking into account poor reporting
https://cmmid.github.io/topics/covid19/severity/global_cfr_estimates.html -
this is a massive over reaction to a none problem the data the government produce proves this is total bullshit. England and Wales flu deaths 32,525 last year (over 20k over 65s just in England alone), US flu deaths 61,000, China flu deaths in the hundreds of thousands, Italy some years ago reported an average of 17,000 flu deaths and that was before the increases in the last couple of year. Corona has been around 60 years, we get new ones every now and then, we have deaths from corona viruses every year, the health people know this, they also know about excess winter mortality which they are not mentioning.
Infection rate is LOWER than for flu, France had last week 175 new flu cases per 100k, this outstrips C.Virus massively, Same in England which had according to the government 14.6 new flu cases per 100k, that's 8300 for that week just in England in ONE WEEK, Scotland flu rates was 27/100k so another 1400+ flu cases in ONE WEEK. England and Wales flu deaths from 2018-19 are 89 on average every single day! Flu rate last winter peaked at 75 cases per 100k, that's 50,000 flu cases in a week.
All data is from the excess winter mortality document from 2018-19 on the .gov website see Tables 6a and 6b, download 6b to see the number of weekly flu deaths.(C.virus is added up for all weeks which is not how you report correctly)
https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/deaths/bulletins/excesswintermortalityinenglandandwales/2018to2019provisionaland2017to2018final#weekly-deaths-and-influenza-activityAlso Watch, listen and understand as to why these deaths are being taken totally out of context!!
this is similar to Jake Olivier counting head injuries in hospitals including those that aren't preventable by helmets (such as cut lips) and ignoring the background head injuries and deaths from motorists and pedestrians and then stating helmets are required for cyclists only.https://www.youtube.com/watch?v=p_AyuhbnPOI
1 Attachment
-
-
More testing for a specific thing gives you more positives than what you aren't testing for, so if you test more for C.19 then you will of course get more +ve results.
Even despite that the self reporting (which is massively under the actual number of people contracting flu) influenza rates are still massively higher than that for C.19 in every countries data that I've looked for.
Also the number of C.19 cases are seemingly being used as an aggregate, not taken as a weeks worth as per the government and indeed WHO method of reporting cases per 100k for influenza, this massively distorts the figures even more especially during peak times of an outbreak.
 Chalfie
Chalfie russmeyer
russmeyer greentricky
greentricky Velocio
Velocio dubtap
dubtap Howard
Howard skydancer
skydancer Scoot
Scoot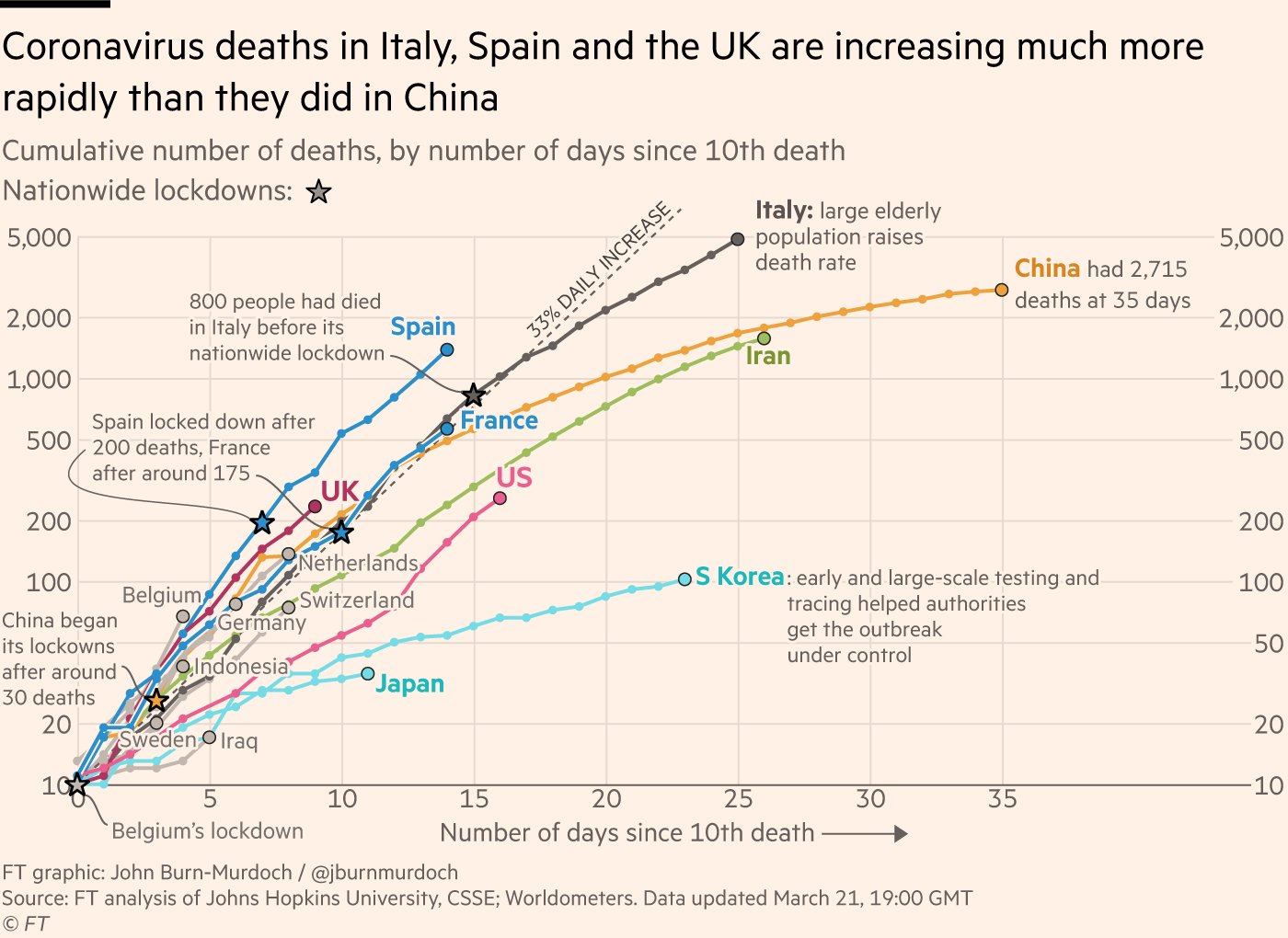
 user62119
user62119 miro_o
miro_o xDOMx
xDOMx h2o
h2o Mr_Bump
Mr_Bump
About
Science, Statistics and Studies [SARS-CoV-2]
Posted by


I read a rebuttal to that ionaddis piece.
He's good and has form in "all scientific research is wrong as it's not reproducible!" I can't find his plos paper.